Golfer's Elbow

Non-traumatic elbow pain can be of various causes. Although
tennis elbow is the commonest but other problems like golfer's elbow, student's
elbow (olecranon bursitis), javelin throwers elbow (sprain injury of the ulnar collateral ligament of the medial elbow) and writer's elbow (ulnar nerve entrapment) are the other leading causes apart from Rheumatoid
arthritis and
referred pain.Sir Douglas Robert Steuart Bader was a Royal Air Force fighter pilot
during the Second World War. He lost his lower limb during the war and started
playing lawn several outdoor games in a wheelchair, lately became a famous golf
player. Famous author Mr A A Gill mentioned in his writing that he is suffering
from golfrr's elbow which he found similar with Douglas Bader. Same like tennis
elbow, it not only occurs to golf players but can also seen in bowling players,
rock climbers (Climber's Elbow) and baseball players (Pitcher's Elbow) or any
other game which is very grip intensive including tennis.
What is Golfer's elbow
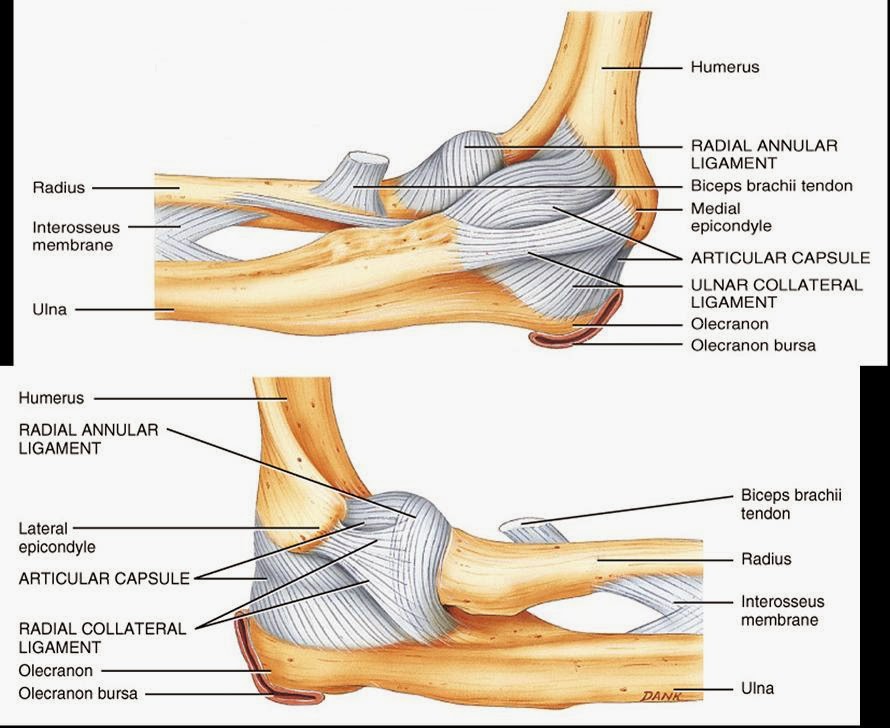
Golfer's elbow or medial epicondylitis is an inflammatory condition of the medial humeral epicondyle-common origin of flexor tendons of the forearm at elbow. Overuse of the wrist flexors causes pain on the
inner side of the elbow.
Treating Golfer's elbow
Untreated golfer’s elbows can last anywhere from 6 months to 2 years. You are also prone to recurrence. Golfer's elbow is a problem
that usually heals with simple treatment, and does not cause any long-term
elbow problems. Treatment is rarely surgical, as this condition is well managed
with a little rest and proper rehabilitation. Before therapy can commence, R.I.C.E.protocol (rest, ice,
compression and elevation)
will typically be used. This protocol helps
to decrease the pain and inflammation. Before steroids and anesthetics are used,
conservative treatment with a physiotherapist
may be attempted. Physiotherapy treatment can
include gentle mobilisation of your neck and elbow joints, electrotherapy,
protective strapping, muscle stretches, neural mobilization, massage and strengthening. Physiotherapy has been shown to be effective in the short and
long-term management of Golfer’s elbow. The
overall prognosis is good. Few patients will need to progress to steroid
injection and even fewer, less than 10%, will need surgical intervention. Aims of the physiotherapy will be:
- Reduction of elbow pain.
- Facilitation of tissue repair.
- Restoration of normal joint range of motion and function.
- Restoration of normal muscle length, strength and movement patterns.
- Normalization of your upper limb neuro-dynamics.
- Normalization of cervical joint function.
Electrotherapy includes application of
Ultrasound : it transmits sound waves through the tissues stimulating the body’s chemical reactions and therefore healing process. It reduces tissue spasm, accelerates the healing process and results in pain relief. If the pain is truly localized well above and away from the ulnar nerve then maybe we’ll consider US using a small sound head, pulsed 50%, 0.5 w/cm square for 5 mins.
LASER : it emits beams of light into the tissues of the body, stimulating chemical reactions and having a similar effect to ultrasound though using light energy instead of sound energy. The course of LASER is divided into 3 phases. The tender part of the musculature and ligament of the medial side with a dosage of 1-2 J per point in the first phase. In the second phase 4-6 J per point is applied for the deeper muscles finally the sore epicondyle itself will treated with dosage of 8-20 J per point. Total dosage will be 30-50 J for 1-4 days per week for 3-5 weeks.
Interferential current : I.F.T introduces a small electrical current into the tissues and can be used at varying frequencies for differing treatment effects. E.g. pain relief, muscle or nerve stimulation, promoting blood flow and reducing swelling/inflammation.
Interferential current : I.F.T introduces a small electrical current into the tissues and can be used at varying frequencies for differing treatment effects. E.g. pain relief, muscle or nerve stimulation, promoting blood flow and reducing swelling/inflammation.
Exercise programs will
include various exercises of muscle
and tendon for reconditioning, starting with
stretching exercises
and gradual strengthening of the flexor-pronator muscles. You may do the stretching exercises right away. You may do the strengthening exercises when stretching is nearly painless. Exercises
should not cause pain, and if they do the exercises should not be done until
the pain resolves.
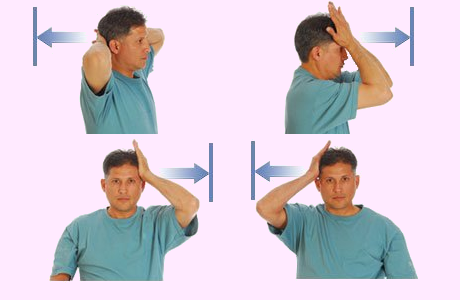
Stretching
Wrist active range of motion:
Flexion and extension: Bend the wrist of your injured arm
forward and back as far as you can. Do 2 sets of 15.
Forearm stretch or Wrist stretch: Press the back of the hand on your injured side
with your other hand to help bend your wrist. Hold for 15 to 30 seconds. Next,
stretch the hand back by pressing the fingers in a backward direction. Hold for
15 to 30 seconds. Keep the arm on your injured side straight during this
exercise. Do 3 sets.
Forearm pronation and
supination: Bend the elbow of your injured arm 90 degrees,
keeping your elbow at your side. Turn your palm up and hold for 5 seconds. Then
slowly turn your palm down and hold for 5 seconds. Make sure you keep your
elbow at your side and bent 90 degrees while you do the exercise. Do 2 sets of
15.
Strengthening
By strengthening the muscles and tendons involved with
golfers' elbow, you can help prevent the problem from returning. Strengthening
will slowly begin with isometrics and progresses to eccentric
exercises helping to extend the range of motion back to where it once was.
After the strengthening exercises, it is common for the patient to ice the area.
Eccentric wrist flexion: Hold
a can or hammer handle in the hand of your injured side with your palm up. Use
the hand on the side that is not injured to bend your wrist up. Then let go of
your wrist and use just your injured side to lower the weight slowly back to
the starting position. Do 3 sets of 15. Gradually increase the weight you are
holding.
Eccentric wrist extension: Hold
a soup can or hammer handle in the hand of your injured side with your palm
facing down. Use the hand on the side that is not injured to bend your wrist
up. Then let go of your wrist and use just your injured side to lower the
weight slowly back to the starting position. Do 3 sets of 15. Gradually
increase the weight you are holding.
Grip strengthening: Squeeze
a soft rubber ball and hold the squeeze for 5 seconds. Do 2 sets of 15.
Forearm pronation and
supination strengthening: Hold a soup can or hammer handle in
your hand and bend your elbow 90 degrees. Slowly turn your hand so your palm is
up and then down. Do 2 sets of 15.
Resisted elbow flexion and
extension: Hold a can of soup with your palm up. Slowly bend
your elbow so that your hand is coming toward your shoulder. Then lower it
slowly so your arm is completely straight. Do 2 sets of 15. Slowly increase the
weight you are using.

A counter-force brace or "elbow strap" to
reduce strain at the elbow epicondyle, to limit pain provocation and to protect
against further damage. A strap with a pad can be placed anteromedially on the proximal forearm.
 |
| Elbow strap |
The
splint is made in 30–45 degrees of elbow flexion. A daytime elbow pad also may
be useful, by limiting additional trauma to the nerve.
 |
| Elbow brace |
Massage : It includes a variety of techniques
and is given with sufficient pressure through the superficial tissue to
reach the deep lying structures. It is used to increase blood flow,
decrease swelling, reduce muscle spasm and promote normal tissue repair.
Deep friction massage : It is an aggressive massage
technique. It is applied across the tissue fibers. Pressure
is given as deeply as possible. This technique is initially painful but can
cause a numbing effect. It can be used to break down scar tissue, restore
normal movement and prepare the injured structure for mobilisation or
manipulation.
Taping may be used if thought necessary to restrict abnormal movement and prevent further damage specially for sports person.
 |
| Taping in Golfer's elbow |
Lifestyle Modification
Lifestyle modification is important specially for the athletes, often a change in technique can resolve the problem. Golf clubs should be sized properly, including grip size. Swing mechanics should be evaluated to ensure patients are swinging properly. Ensure that your workstation ergonomics helps you to attain good posture and keep the arm close to the body.Medication
Both anesthetics and steroids are used to
treat this condition. Simple analgesic medication has a place, as
does more specific treatment with oral anti-inflammatory medications
(NSAIDs : ibuprofen, naproxen or aspirin).
These will help control pain and any inflammation. A more invasive
treatment is the injection into and around the inflamed and tender area of a
long-acting glucocorticoid (steroid)
agent. The ulnar nerve runs in the groove between the
medial humeral epicondyle and the olecranon
process of the ulna. It is most important that this nerve should not be
damaged accidentally in the process of injecting a golfer's elbow. After
causing an initial exacerbation of symptoms lasting 24 to 48 hours, this may
produce a resolution of the condition in some five to seven days.
Surgical intervention
If all else fails, epicondylar debridement may be effective. The ulnar nerve may also be
decompressed surgically.

.jpg)
Very Nice Post. I am very happy to see this post. Such a wonderful information to share with us. I would like to share with my friends. For more information visit here digital goniometer
ReplyDelete